The Best Way To Diagnose Calcaneal Apophysitis?
Overview
The calcaneal apophysis is a growth center where the Achilles tendon and the plantar fascia attach to the heel. It first appears in children aged 7 to 8 years. By ages 12 to 14 years the growth center matures and fuses to the heel bone. Injuries can occur from excessive tension on the Achilles tendon and the plantar fascia, or from direct impact on the heel. Excessive stress on this growth center can cause irritation of the heel, also called Sever?s disease.
Causes
Physically active children run the risk of developing Sever?s disease because they put the most strain on their growing bones. Sever?s usually occurs during the adolescent growth spurt, when young people grow most rapidly. (This growth spurt can begin any time between the ages of 8 and 13 for girls and 10 and 15 for boys.) By age 15 the back of the heel usually finished growing. As teens grow, the growth plates harden and the growing bones fuse together into mature bone. Young people engaged in physical activities and sports that involve jumping and running on hard surfaces-such as track, basketball, soccer, and gymnastics-are ata higher risk for developing Sever?s disease. Poor-fitting shoes can contribute by not providing enough support or padding for the feet or by rubbing against the back of the heel.
Symptoms
The symptoms of Sever?s disease occur in the heel and the foot, and may worsen with activity. Pain and stiffness can occur in one or both heels. Symptoms can include. Swelling in the heel. Redness in the heel. Antalgic gait (such as limping). Foot pain or stiffness first thing in the morning or while walking. Pain that is worsened by squeezing the heel.
Diagnosis
Your Podiatrist or Physiotherapist will assist in diagnosing the injury and the extent of the damage. From this, they will develop a management plan which may include rest or activity modification, soft tissue treatment such as massage and stretching, correction of biomechanics through heel raises or orthoses and the progression through a series of specific strengthening exercises.
Non Surgical Treatment
First, your child should cut down or stop any activity that causes heel pain. Apply ice to the injured heel for 25 minutes three times a day. Your child should not go barefoot. If your child has severe heel pain, ibuprofen (Advil) will help. It is important that your child performs exercises to stretch the hamstring and calf muscles, and the tendons on the back of the leg. The child should do these stretches five times each, two or three times a day. Each stretch should be held for 20 seconds. Your child also needs to do exercises to strengthen the muscles on the front of the shin. To do this, have your child stand facing a wall to stretch the calves and the heel cord. Place one foot a shoulder?s width in front of the other, both feet facing the wall. The front knee is bent and the back knee is straight during the calf stretch. Then have your child push against the wall and feel the stretch in his or her back leg. To stretch out the heel cord, have him or her stay in the same position and bend the back knee. Repeat three times. Practice this stretch twice daily.
The calcaneal apophysis is a growth center where the Achilles tendon and the plantar fascia attach to the heel. It first appears in children aged 7 to 8 years. By ages 12 to 14 years the growth center matures and fuses to the heel bone. Injuries can occur from excessive tension on the Achilles tendon and the plantar fascia, or from direct impact on the heel. Excessive stress on this growth center can cause irritation of the heel, also called Sever?s disease.
Causes
Physically active children run the risk of developing Sever?s disease because they put the most strain on their growing bones. Sever?s usually occurs during the adolescent growth spurt, when young people grow most rapidly. (This growth spurt can begin any time between the ages of 8 and 13 for girls and 10 and 15 for boys.) By age 15 the back of the heel usually finished growing. As teens grow, the growth plates harden and the growing bones fuse together into mature bone. Young people engaged in physical activities and sports that involve jumping and running on hard surfaces-such as track, basketball, soccer, and gymnastics-are ata higher risk for developing Sever?s disease. Poor-fitting shoes can contribute by not providing enough support or padding for the feet or by rubbing against the back of the heel.
Symptoms
The symptoms of Sever?s disease occur in the heel and the foot, and may worsen with activity. Pain and stiffness can occur in one or both heels. Symptoms can include. Swelling in the heel. Redness in the heel. Antalgic gait (such as limping). Foot pain or stiffness first thing in the morning or while walking. Pain that is worsened by squeezing the heel.
Diagnosis
Your Podiatrist or Physiotherapist will assist in diagnosing the injury and the extent of the damage. From this, they will develop a management plan which may include rest or activity modification, soft tissue treatment such as massage and stretching, correction of biomechanics through heel raises or orthoses and the progression through a series of specific strengthening exercises.
Non Surgical Treatment
First, your child should cut down or stop any activity that causes heel pain. Apply ice to the injured heel for 25 minutes three times a day. Your child should not go barefoot. If your child has severe heel pain, ibuprofen (Advil) will help. It is important that your child performs exercises to stretch the hamstring and calf muscles, and the tendons on the back of the leg. The child should do these stretches five times each, two or three times a day. Each stretch should be held for 20 seconds. Your child also needs to do exercises to strengthen the muscles on the front of the shin. To do this, have your child stand facing a wall to stretch the calves and the heel cord. Place one foot a shoulder?s width in front of the other, both feet facing the wall. The front knee is bent and the back knee is straight during the calf stretch. Then have your child push against the wall and feel the stretch in his or her back leg. To stretch out the heel cord, have him or her stay in the same position and bend the back knee. Repeat three times. Practice this stretch twice daily.
Adult Aquired Flat Feet Cause And Treatment
Overview
Acquired adult flatfoot deformity (AAFD) is a progressive flattening of the arch of the foot that occurs as the posterior tibial tendon becomes insufficient. It has many other names such posterior tibial tendon dysfunction, posterior tibial tendon insufficiency and dorsolateral peritalar subluxation. This problem may progress from early stages with pain along the posterior tibial tendon to advanced deformity and arthritis throughout the hindfoot and ankle. 
Causes
Damage to the posterior tendon from overuse is the most common cause for adult acquired flatfoot. Running, walking, hiking, and climbing stairs are activities that add stress to this tendon, and this overuse can lead to damage. Obesity, previous ankle surgery or trauma, diabetes (Charcot foot), and rheumatoid arthritis are other common risk factors.
Symptoms
Patients often experience pain and/or deformity at the ankle or hindfoot. When the posterior tibial tendon does not work properly, a number of changes can occur to the foot and ankle. In the earlier stages, symptoms often include pain and tenderness along the posterior tibial tendon behind the inside of the ankle. As the tendon progressively fails, deformity of the foot and ankle may occur. This deformity can include progressive flattening of the arch, shifting of the heel so that it no longer is aligned underneath the rest of the leg, rotation and deformity of the forefoot, tightening of the heel cord, development of arthritis, and deformity of the ankle joint. At certain stages of this disorder, pain may shift from the inside to the outside aspect of the ankle as the heel shifts outward and structures are pinched laterally.
Diagnosis
Looking at the patient when they stand will usually demonstrate a flatfoot deformity (marked flattening of the medial longitudinal arch). The front part of the foot (forefoot) is often splayed out to the side. This leads to the presence of a ?too many toes? sign. This sign is present when the toes can be seen from directly behind the patient. The gait is often somewhat flatfooted as the patient has the dysfunctional posterior tibial tendon can no longer stabilize the arch of the foot. The physician?s touch will often demonstrate tenderness and sometimes swelling over the inside of the ankle just below the bony prominence (the medial malleolus). There may also be pain in the outside aspect of the ankle. This pain originates from impingement or compression of two tendons between the outside ankle bone (fibula) and the heel bone (calcaneus) when the patient is standing.
Non surgical Treatment
Nonoperative treatment of posterior tibial tendon dysfunction can be successful with the Arizona AFO brace, particularly when treatment is initiated in the early stages of the disease. This mandates that the orthopedist has a high index of suspicion when evaluating patients to make an accurate diagnosis. Although there is a role for surgical management of acquired flat feet, a well-fitted, custom-molded leather and polypropylene orthosis can be effective at relieving symptoms and either obviating or delaying any surgical intervention. In today's climate of patient satisfaction directed health care, a less invasive treatment modality that relieves pain may prove to be more valuable than similar pain relief that is obtained after surgery. Questions regarding the long-term results of bracing remain unanswered. Future studies are needed to determine if disease progression and arthrosis occur despite symptomatic relief with a brace. Furthermore, age- and disease stage-matched control groups who are randomized to undergo surgery or bracing are necessary to compare these different treatment modalities. 
Surgical Treatment
If conservative treatment fails surgical intervention is offered. For a Stage 1 deformity a posterior tibial tendon tenosynovectomy (debridement of the tendon) or primary repair may be indicated. For Stage 2 a combination of Achilles lengthening with bone cuts, calcaneal osteotomies, and tendon transfers is common. Stage 2 flexible PTTD is the most common stage patients present with for treatment. In Stage 3 or 4 PTTD isolated fusions, locking two or more joints together, maybe indicated. All treatment is dependent on the stage and severity at presentation with the goals and activity levels of the patient in mind. Treatment is customized to the individual patient needs.
Heel Soreness
Overview

There are two categories of Heel Pain. pain on the bottom (plantar) and pain on the back of the heel bone (calcaneus). The most common cause pain on the bottom of the heel is plantar fasciitis or better known as heel spur syndrome. Another common cause is nerve entrapment (~70% of patients have both plantar fasciitis and nerve entrapment) and less commonly, stress fracture, arthritis, tendonitis, a cyst or a combination of these. Pain on the back of the heel most often involves the insertion of the Achilles tendon into the bone. Due to the multi-factorial nature of heel pain, the earlier a diagnosis is made, the better the outcome.
Causes
Some of the many causes of heel pain can include abnormal walking style (such as rolling the feet inwards), obesity, ill-fitting shoes eg narrow toe, worn out shoes, standing, running or jumping on hard surfaces, recent changes in exercise program, heel trauma eg. stress fractures, bursitis (inflammation of a bursa), health disorders, including diabetes and arthritis.
Symptoms
Symptoms include a dull ache which is felt most of the time with episodes of a sharp pain in the centre of the heel or on the inside margin of the heel. Often the pain is worse on first rising in the morning and after rest and is aggravated by prolonged weight bearing & thin soled shoes.
Diagnosis
In most cases, your GP or a podiatrist (a specialist in foot problems and foot care) should be able to diagnose the cause of your heel pain by asking about your symptoms and medical history, examining your heel and foot.
Non Surgical Treatment
If you develop heel pain, you can try several methods at home to ease your discomfort. For example rest as much as possible, apply ice to the heel for 10 to 15 minutes twice a day, use over-the-counter pain medications, wear shoes that fit properly, wear night splints, a special device that stretches the foot while you sleep, use heel cups or shoe inserts to reduce pain, If these home care strategies do not ease your pain, you will need to see your doctor. He or she will perform a physical exam and ask you about your symptoms and when they began. Your doctor may also take an X-ray to determine the cause of your heel pain. Once your doctor knows what is causing your pain, he or she will be able to provide you with the appropriate treatment. In many cases, your doctor may prescribe physical therapy. This can help to strengthen the muscles and tendons in your foot, which helps to prevent further injury. If your pain is severe, your doctor may provide you with anti-inflammatory medications. These medications can be injected into the foot or taken by mouth. Your doctor may also recommend that you support your foot as much as possible-either by taping the foot or by using special footwear devices. In very rare cases, your doctor may recommend surgery to correct the problem. However, heel surgery often requires a long recovery time and may not always relieve your foot pain.
Surgical Treatment
With the advancements in technology and treatments, if you do need to have surgery for the heel, it is very minimal incision that?s done. And the nice thing is your recovery period is short and you should be able to bear weight right after the surgery. This means you can get back to your weekly routine in just a few weeks. Recovery is a lot different than it used to be and a lot of it is because of doing a minimal incision and decreasing trauma to soft tissues, as well as even the bone. So if you need surgery, then your recovery period is pretty quick.
Prevention

It may not be possible to prevent all cases of heel pain. However, there are some easy steps that you can take to avoid injury to the heel and prevent pain. Whenever possible, you should wear shoes that fit properly and support the foot, wear the right shoes for physical activity, stretch your muscles before exercising, pace yourself during physical activity, maintain a healthy diet, rest when you feel tired or when your muscles ache, maintain a healthy weight.
There are two categories of Heel Pain. pain on the bottom (plantar) and pain on the back of the heel bone (calcaneus). The most common cause pain on the bottom of the heel is plantar fasciitis or better known as heel spur syndrome. Another common cause is nerve entrapment (~70% of patients have both plantar fasciitis and nerve entrapment) and less commonly, stress fracture, arthritis, tendonitis, a cyst or a combination of these. Pain on the back of the heel most often involves the insertion of the Achilles tendon into the bone. Due to the multi-factorial nature of heel pain, the earlier a diagnosis is made, the better the outcome.
Causes
Some of the many causes of heel pain can include abnormal walking style (such as rolling the feet inwards), obesity, ill-fitting shoes eg narrow toe, worn out shoes, standing, running or jumping on hard surfaces, recent changes in exercise program, heel trauma eg. stress fractures, bursitis (inflammation of a bursa), health disorders, including diabetes and arthritis.
Symptoms
Symptoms include a dull ache which is felt most of the time with episodes of a sharp pain in the centre of the heel or on the inside margin of the heel. Often the pain is worse on first rising in the morning and after rest and is aggravated by prolonged weight bearing & thin soled shoes.
Diagnosis
In most cases, your GP or a podiatrist (a specialist in foot problems and foot care) should be able to diagnose the cause of your heel pain by asking about your symptoms and medical history, examining your heel and foot.
Non Surgical Treatment
If you develop heel pain, you can try several methods at home to ease your discomfort. For example rest as much as possible, apply ice to the heel for 10 to 15 minutes twice a day, use over-the-counter pain medications, wear shoes that fit properly, wear night splints, a special device that stretches the foot while you sleep, use heel cups or shoe inserts to reduce pain, If these home care strategies do not ease your pain, you will need to see your doctor. He or she will perform a physical exam and ask you about your symptoms and when they began. Your doctor may also take an X-ray to determine the cause of your heel pain. Once your doctor knows what is causing your pain, he or she will be able to provide you with the appropriate treatment. In many cases, your doctor may prescribe physical therapy. This can help to strengthen the muscles and tendons in your foot, which helps to prevent further injury. If your pain is severe, your doctor may provide you with anti-inflammatory medications. These medications can be injected into the foot or taken by mouth. Your doctor may also recommend that you support your foot as much as possible-either by taping the foot or by using special footwear devices. In very rare cases, your doctor may recommend surgery to correct the problem. However, heel surgery often requires a long recovery time and may not always relieve your foot pain.
Surgical Treatment
With the advancements in technology and treatments, if you do need to have surgery for the heel, it is very minimal incision that?s done. And the nice thing is your recovery period is short and you should be able to bear weight right after the surgery. This means you can get back to your weekly routine in just a few weeks. Recovery is a lot different than it used to be and a lot of it is because of doing a minimal incision and decreasing trauma to soft tissues, as well as even the bone. So if you need surgery, then your recovery period is pretty quick.
Prevention
It may not be possible to prevent all cases of heel pain. However, there are some easy steps that you can take to avoid injury to the heel and prevent pain. Whenever possible, you should wear shoes that fit properly and support the foot, wear the right shoes for physical activity, stretch your muscles before exercising, pace yourself during physical activity, maintain a healthy diet, rest when you feel tired or when your muscles ache, maintain a healthy weight.
The Primary Causes And Treatment Plans Of Achilles Tendinitis
Overview
 Achilles tendinitis is an overuse injury of the Achilles tendon, the band of tissue that connects calf muscles at the back of the lower leg to your heel bone. Achilles tendinitis most commonly occurs in runners who have suddenly increased the intensity or duration of their runs. It's also common in middle-aged people who play sports, such as tennis or basketball, only on the weekends. Most cases of Achilles tendinitis can be treated with relatively simple, at-home care under your doctor's supervision. Self-care strategies are usually necessary to prevent recurring episodes. More-serious cases of Achilles tendinitis can lead to tendon tears (ruptures) that may require surgical repair.
Achilles tendinitis is an overuse injury of the Achilles tendon, the band of tissue that connects calf muscles at the back of the lower leg to your heel bone. Achilles tendinitis most commonly occurs in runners who have suddenly increased the intensity or duration of their runs. It's also common in middle-aged people who play sports, such as tennis or basketball, only on the weekends. Most cases of Achilles tendinitis can be treated with relatively simple, at-home care under your doctor's supervision. Self-care strategies are usually necessary to prevent recurring episodes. More-serious cases of Achilles tendinitis can lead to tendon tears (ruptures) that may require surgical repair.
Causes
There are a number of causes and risk factors associated with Achilles Tendinitis. One of the most common causes is simply a lack of conditioning. If the tendon, and muscles that connect to the tendon, have not been trained or conditioned, this can lead to a weakness that may result in an Achilles injury. Overtraining is also associated with Achilles Tendinitis. Doing too much, too soon places excessive strain on the Achilles tendon and doesn't allow the tendon enough time to recovery properly. Over time small tears and general degeneration result in a weakening of the tendon, which leads to inflammation and pain. Other causes of Achilles injury include a lack of warming up and stretching. Wearing inadequate footwear, running or training on uneven ground, and simply standing on, or in something you're not meant to. Biomechanical problems such as high arched feet or flat feet can also lead to Achilles injuries.
Symptoms
The pain associated with Achilles tendonitis can come on gradually or be caused by some type of leg or foot trauma. The pain can be a shooting, burning, or a dull ache. You can experience the pain at either the insertion point on the back of the heel or upwards on the Achilles tendon within a few inches. Swelling is also common along the area with the pain. The onset of discomfort at the insertion can cause a bump to occur called a Haglund's deformities or Pump bump. This can be inflammation in the bursa sac that surrounds the insertion of the Achilles tendon, scar tissue from continuous tares of the tendon, or even some calcium buildup. In this situation the wearing of closed back shoes could irritate the bump. In the event of a rupture, which is rare, the foot will not be able to go through the final stage of push off causing instability. Finally, you may experience discomfort, even cramping in the calf muscle.
Diagnosis
Confirming Achilles tendonitis may involve imaging tests. X-rays provide images of the bones of the foot and leg. Magnetic resonance imaging (MRI) is useful for detecting ruptures and degeneration of tissue. Ultrasound shows tendon movement, related damage, and inflammation.
Nonsurgical Treatment
There are a variety of treatments for Achilles tendonitis. These range from rest and aspirin to steroid injections and surgery. Your doctor might suggest, reducing your physical activity, stretching and strengthening the calf muscles, switching to a different, less strenuous sport, icing the area after exercise or when in pain, raising your foot to decrease swelling, wearing a brace or compressive elastic bandage to prevent heel movement, undergoing physical therapy, taking anti-inflammatory medication (e.g., aspirin or ibuprofen) for a limited time, getting steroid injections, Sometimes more conservative treatments are not effective. In these cases, surgery may be necessary to repair the Achilles tendon. If the condition intensifies and is left untreated, there?s a greater risk of an Achilles rupture. This can cause sharp pain in the heel area.

Surgical Treatment
Your doctor may recommend surgery if, after around six months, other treatments haven?t worked and your symptoms are having an impact on your day-to-day life. Surgery involves removing damaged areas of your tendon and repairing them.
Prevention
By properly training the body, an athlete can build the strength of their tendons and muscles. Following a workout and dieting plan, the body will be able to build muscle and strengthen most effectively. Additionally, doing the following can prevent tendinitis. Wearing appropriate shoes will give your foot the support it needs for proper movements of the foot and ankle. Improper movements will put additional stress on your body. Stretching before an athletic activity, Stretching primes the body for a taxing activity. Additionally, this will get your blood flowing and reduce the risk of pulling a muscle. Ask your doctor about orthotics, Custom orthotics can help get your foot into proper alignment. If the foot does not execute proper mechanics, the body will adjust which will cause pain and increase the chances of injury.
Achilles tendinitis is an overuse injury of the Achilles tendon, the band of tissue that connects calf muscles at the back of the lower leg to your heel bone. Achilles tendinitis most commonly occurs in runners who have suddenly increased the intensity or duration of their runs. It's also common in middle-aged people who play sports, such as tennis or basketball, only on the weekends. Most cases of Achilles tendinitis can be treated with relatively simple, at-home care under your doctor's supervision. Self-care strategies are usually necessary to prevent recurring episodes. More-serious cases of Achilles tendinitis can lead to tendon tears (ruptures) that may require surgical repair.
Causes
There are a number of causes and risk factors associated with Achilles Tendinitis. One of the most common causes is simply a lack of conditioning. If the tendon, and muscles that connect to the tendon, have not been trained or conditioned, this can lead to a weakness that may result in an Achilles injury. Overtraining is also associated with Achilles Tendinitis. Doing too much, too soon places excessive strain on the Achilles tendon and doesn't allow the tendon enough time to recovery properly. Over time small tears and general degeneration result in a weakening of the tendon, which leads to inflammation and pain. Other causes of Achilles injury include a lack of warming up and stretching. Wearing inadequate footwear, running or training on uneven ground, and simply standing on, or in something you're not meant to. Biomechanical problems such as high arched feet or flat feet can also lead to Achilles injuries.
Symptoms
The pain associated with Achilles tendonitis can come on gradually or be caused by some type of leg or foot trauma. The pain can be a shooting, burning, or a dull ache. You can experience the pain at either the insertion point on the back of the heel or upwards on the Achilles tendon within a few inches. Swelling is also common along the area with the pain. The onset of discomfort at the insertion can cause a bump to occur called a Haglund's deformities or Pump bump. This can be inflammation in the bursa sac that surrounds the insertion of the Achilles tendon, scar tissue from continuous tares of the tendon, or even some calcium buildup. In this situation the wearing of closed back shoes could irritate the bump. In the event of a rupture, which is rare, the foot will not be able to go through the final stage of push off causing instability. Finally, you may experience discomfort, even cramping in the calf muscle.
Diagnosis
Confirming Achilles tendonitis may involve imaging tests. X-rays provide images of the bones of the foot and leg. Magnetic resonance imaging (MRI) is useful for detecting ruptures and degeneration of tissue. Ultrasound shows tendon movement, related damage, and inflammation.
Nonsurgical Treatment
There are a variety of treatments for Achilles tendonitis. These range from rest and aspirin to steroid injections and surgery. Your doctor might suggest, reducing your physical activity, stretching and strengthening the calf muscles, switching to a different, less strenuous sport, icing the area after exercise or when in pain, raising your foot to decrease swelling, wearing a brace or compressive elastic bandage to prevent heel movement, undergoing physical therapy, taking anti-inflammatory medication (e.g., aspirin or ibuprofen) for a limited time, getting steroid injections, Sometimes more conservative treatments are not effective. In these cases, surgery may be necessary to repair the Achilles tendon. If the condition intensifies and is left untreated, there?s a greater risk of an Achilles rupture. This can cause sharp pain in the heel area.
Surgical Treatment
Your doctor may recommend surgery if, after around six months, other treatments haven?t worked and your symptoms are having an impact on your day-to-day life. Surgery involves removing damaged areas of your tendon and repairing them.
Prevention
By properly training the body, an athlete can build the strength of their tendons and muscles. Following a workout and dieting plan, the body will be able to build muscle and strengthen most effectively. Additionally, doing the following can prevent tendinitis. Wearing appropriate shoes will give your foot the support it needs for proper movements of the foot and ankle. Improper movements will put additional stress on your body. Stretching before an athletic activity, Stretching primes the body for a taxing activity. Additionally, this will get your blood flowing and reduce the risk of pulling a muscle. Ask your doctor about orthotics, Custom orthotics can help get your foot into proper alignment. If the foot does not execute proper mechanics, the body will adjust which will cause pain and increase the chances of injury.
What Is Pain Under The Heel And Simple Tips To Alleviate It

Overview
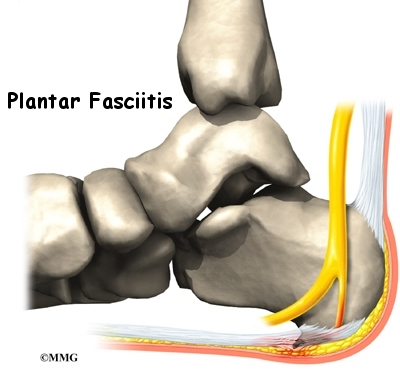
Plantar fasciitis is that pain in the bottom of your foot usually in the heel. That pain hurts especially with the first few steps in the morning as you get out of bed. This strange name comes from: "Plantar" means something that belongs to the foot, "fascia" means a band or ligament or a connective tissue, and "itis" means inflammation. You can see in the picture the plantar fascia band as it runs along the foot. This band connects your heel bone to the toes.
Causes
There are a number of plantar fasciitis causes. The plantar fascia ligament is like a rubber band and loosens and contracts with movement. It also absorbs significant weight and pressure. Because of this function, plantar fasciitis can easily occur from a number of reasons. Among the most common is an overload of physical activity or exercise. Athletes are particularly prone to plantar fasciitis and commonly suffer from it. Excessive running, jumping, or other activities can easily place repetitive or excessive stress on the tissue and lead to tears and inflammation, resulting in moderate to severe pain. Athletes who change or increase the difficulty of their exercise routines are also prone to overdoing it and causing damage. Another common cause of plantar fasciitis is arthritis. Certain types of arthritis can cause inflammation to develop in tendons, resulting in plantar fasciitis. This cause is particularly common among elderly patients. Diabetes is also a factor that can contribute to further heel pain and damage, particularly among the elderly. Among the most popular factors that contribute to plantar fasciitis is wearing incorrect shoes. In many cases, shoes either do not fit properly, or provide inadequate support or cushioning. While walking or exercising in improper shoes, weight distribution becomes impaired, and significantly stress can be added to the plantar fascia ligament.
Symptoms
Pain tends to start gradually, often just in the heel, but it can sometimes be felt along the whole of the plantar fascia. The symptoms are initially worse in the morning and mostly after, rather than during, activity. As the condition becomes worse, the symptoms become more persistent.
Diagnosis
Plantar fasciitis is usually diagnosed by a health care provider after consideration of a person’s presenting history, risk factors, and clinical examination. Tenderness to palpation along the inner aspect of the heel bone on the sole of the foot may be elicited during the physical examination. The foot may have limited dorsiflexion due to tightness of the calf muscles or the Achilles tendon. Dorsiflexion of the foot may elicit the pain due to stretching of the plantar fascia with this motion. Diagnostic imaging studies are not usually needed to diagnose plantar fasciitis. However, in certain cases a physician may decide imaging studies (such as X-rays, diagnostic ultrasound or MRI) are warranted to rule out other serious causes of foot pain. Bilateral heel pain or heel pain in the context of a systemic illness may indicate a need for a more in-depth diagnostic investigation. Lateral view x-rays of the ankle are the recommended first-line imaging modality to assess for other causes of heel pain such as stress fractures or bone spur development. Plantar fascia aponeurosis thickening at the heel greater than 5 millimeters as demonstrated by ultrasound is consistent with a diagnosis of plantar fasciitis. An incidental finding associated with this condition is a heel spur, a small bony calcification on the calcaneus (heel bone), which can be found in up to 50% of those with plantar fasciitis. In such cases, it is the underlying plantar fasciitis that produces the heel pain, and not the spur itself. The condition is responsible for the creation of the spur though the clinical significance of heel spurs in plantar fasciitis remains unclear.
Non Surgical Treatment
Plantar fasciitis can be a difficult problem to treat, with no panacea available. Fortunately, most patients with this condition eventually have satisfactory outcomes with nonsurgical treatment. Therefore, management of patient expectations minimizes frustration for both the patient and the provider.

Surgical Treatment
Surgery is rarely used in the treatment of plantar fasciitis. However it may be recommended when conservative treatment has been tried for several months but does not bring adequate relief of symptoms. Surgery usually involves the partial release of the plantar fascia from the heel bone. In approximately 75% of cases symptoms are fully resolved within six months. In a small percentage of cases, symptoms may take up to 12 months to fully resolve.
Prevention
Factors that help prevent plantar fasciitis and reduce the risk of recurrence include. Exercises to strengthen the muscles of the lower leg and ankle. Warming up before commencing physical activity. Maintaining a healthy body weight. Avoiding high heeled footwear. Using orthotic devices such as arch supports and heel raises in footwear, particularly for people with very high arches or flat feet. Daily stretches of plantar fascia and Achilles tendon.
What Triggers Heel Discomfort And Approaches To Prevent It

Overview
If your first few steps out of bed in the morning cause severe pain in the heel of your foot, you may have plantar fasciitis, an overuse injury that affects the sole of the foot. A diagnosis of plantar fasciitis means you have inflamed the tough, fibrous band of tissue (fascia) connecting your heel bone to the base of your toes.
Causes
Patients with tight calf muscles will suffer with excessive pulling of the muscle group on the back of the heel. This in turn creates pulling of other structures that are attached to the heel, including the Plantar Fascia. When the pulling continues for long enough, then inflammation will develop and lead to Plantar Fasciitis. This causes Heel Pain. It is extremely common for patients who increase their level of activity to develop Plantar Fasciitis. Boot camp, running, zumba, recreational walking or other quick movement sports such as tennis or touch football are typical causes of Heel Pain. The sharp increase in exercise is too much for the foot to cope with and the stress on the Plantar Fascia causes inflammation. The Heel Pain that is caused by this inflammation is known as Plantar Fasciitis.
Symptoms
When plantar fasciitis occurs, the pain is typically sharp and usually unilateral (70% of cases).Heel pain worsens by bearing weight on the heel after long periods of rest. Individuals with plantar fasciitis often report their symptoms are most intense during their first steps after getting out of bed or after prolonged periods of sitting. Improvement of symptoms is usually seen with continued walking. Numbness, tingling, swelling, or radiating pain are rare but reported symptoms. If the plantar fascia continues to be overused in the setting of plantar fasciitis, the plantar fascia can rupture. Typical signs and symptoms of plantar fascia rupture include a clicking or snapping sound, significant local swelling, and acute pain in the sole of the foot.
Diagnosis
Most cases of plantar fasciitis are diagnosed by a health care provider who listens carefully to your description of symptoms. During an examination of your feet, your health care provider will have to press on the bottom of your feet, the area most likely to be painful in plantar fasciitis. Because the pain of plantar fasciitis has unique characteristics, pain upon rising, improvement after walking for several minutes, pain produced by pressure applied in a specific location on your foot but not with pressure in other areas, your health care provider will probably feel comfortable making the diagnosis based on your symptoms and a physical examination. Your health care provider may suggest that you have an X-ray of your foot to verify that there is no stress fracture causing your pain.
Non Surgical Treatment
Over-the-counter Orthotics. A soft, over-the-counter orthotic (Prefabricated orthotic) with an accommodating arch support has proven to be quite helpful in the management of plantar fascia symptoms. Studies demonstrate that it is NOT necessary to obtain a custom orthotic for the treatment of this problem. Comfort Shoes. Shoes with a stiff sole, rocker-bottom contour, and a comfortable leather upper combined with an over-the-counter orthotic or a padded heel can be very helpful in the treatment of plantar fasciitis. Anti-Inflammatory Medication (NSAIDs): A short course of over-the-counter anti-inflammatory medications may be helpful in managing plantar fasciitis symptoms providing the patient does not have any contra-indications such as a history of stomach ulcers. Activity Modification Any activity that has recently been started, such as a new running routine or a new exercise at the gym that may have increased loading through the heel area, should be stopped on a temporary basis until the symptoms have resolved. At that point, these activities can be gradually started again. Also, any activity changes (ex. sitting more) that will limit the amount of time a patient is on their feet each day may be helpful. A night splint, which keeps the ankle in a neutral position (right angle) while the patient sleeps, can be very helpful in alleviating the significant morning symptoms. A night splint may be prescribed by your physician. Alternatively, it can be ordered online or even obtained in some medical supply stores. This splint is worn nightly for 1-3 weeks until the cycle of pain is broken. Furthermore, this splinting can be reinstituted for a short period of time is symptoms recur.
Surgical Treatment
Surgery is usually not needed for plantar fasciitis. About 95 out of 100 people who have plantar fasciitis are able to relieve heel pain without surgery. Your doctor may consider surgery if non-surgical treatment has not helped and heel pain is restricting your daily activities. Some doctors feel that you should try non-surgical treatment for at least 6 months before you consider surgery. The main types of surgery for plantar fasciitis are Plantar fascia release. This procedure involves cutting part of the plantar fascia ligament . This releases the tension on the ligament and relieves inflammation . Other procedures, such as removing a heel spur or stretching or loosening specific foot nerves. These surgeries are usually done in combination with plantar fascia release when there is lasting heel pain and another heel problem. Experts in the past thought that heel spurs caused plantar fasciitis. Now experts generally believe that heel spurs are the result, not the cause, of plantar fasciitis. Many people with large heel spurs never have heel pain or plantar fasciitis. So surgery to remove heel spurs is rarely done.
Prevention
Every time your foot strikes the ground, the plantar fascia is stretched. You can reduce the strain and stress on the plantar fascia by following these simple instructions: Avoid running on hard or uneven ground, lose any excess weight, and wear shoes and orthotics that support your arch to prevent over-stretching of the plantar fascia.
What Causes Heel Pain

Overview
The plantar fascia (a connective tissue structure) stretches from the toes and ball of the foot, through the arch, and connects to the heel bone in three places: outside, center and inside. Normally it helps the foot spring as it rolls forward. It also provides support for the arch of the foot. The plantar fascia helps keep the foot on track, cutting down on oscillation. When the foot over-pronates (rolls to the inside) the plantar fascia tries to stabilize it and prevent excessive roll. In time, the inside and sometimes center connections are overstressed and pull away from their attachments. The first sign is usually heel pain as you rise in the morning. When you walk around, the pain may subside, only to return the next morning. Inflammation and increased soreness are the results of long-term neglect and continued abuse. A heel bone spur may develop after a long period of injury when there is no support for the heel. The plantar fascia attaches to the heel bone with small fibers. When these become irritated they become inflamed with blood containing white blood cells. Within the white blood cells are osteoblasts which calcify to form bone spurs and calcium deposits. The body is trying to reduce stress on that area by building a bone in the direction of stress. Unfortunately, these foreign substances cause pain and further irritation in the surrounding soft tissue.
Causes
You're more likely to develop the condition if you're female, overweight or have a job that requires a lot of walking or standing on hard surfaces. You're also at risk if you walk or run for exercise, especially if you have tight calf muscles that limit how far you can flex your ankles. People with very flat feet or very high arches also are more prone to plantar fasciitis.
Symptoms
Plantar fasciitis generally occurs in one foot. Bilateral plantar fasciitis is unusual and tends to be the result of a systemic arthritic condition that is exceptionally rare among athletes. Males suffer from a somewhat greater incidence of plantar fasciitis than females, perhaps as a result of greater weight coupled with greater speed and ground impact, as well as less flexibility in the foot. Typically, the sufferer of plantar fasciitis experiences pain upon rising after sleep, particularly the first step out of bed. Such pain is tightly localized at the bony landmark on the anterior medial tubercle of the calcaneus. In some cases, pain may prevent the athlete from walking in a normal heel-toe gait, causing an irregular walk as means of compensation. Less common areas of pain include the forefoot, Achilles tendon, or subtalar joint. After a brief period of walking, the pain usually subsides, but returns again either with vigorous activity or prolonged standing or walking. On the field, an altered gait or abnormal stride pattern, along with pain during running or jumping activities are tell-tale signs of plantar fasciitis and should be given prompt attention. Further indications of the injury include poor dorsiflexion (lifting the forefoot off the ground) due to a shortened gastroc complex, (muscles of the calf). Crouching in a full squat position with the sole of the foot flat on the ground can be used as a test, as pain will preclude it for the athlete suffering from plantar fasciitis, causing an elevation of the heel due to tension in the gastroc complex.
Diagnosis
X-rays are a commonly used diagnostic imaging technique to rule out the possibility of a bone spur as a cause of your heel pain. A bone spur, if it is present in this location, is probably not the cause of your pain, but it is evidence that your plantar fascia has been exerting excessive force on your heel bone. X-ray images can also help determine if you have arthritis or whether other, more rare problems, stress fractures, bone tumors-are contributing to your heel pain.
Non Surgical Treatment
Careful attention to footwear is critical. Every effort should be made to wear comfortable shoes with proper arch support, fostering proper foot posture. Should arch supports prove insufficient, an orthotic shoe should be considered. Fortunately, most cases of plantar fasciitis respond well to non-operative treatment. Recovery times however vary enormously from one athlete to another, depending on age, overall health and physical condition as well as severity of injury. A broad period between 6 weeks and 6 months is usually sufficient for proper healing. Additionally, the mode of treatment must be flexible depending on the details of a particular athlete’s injury. Methods that prove successful in one patient, may not improve the injury in another. Early treatment typically includes the use of anti-inflammatory medication, icing, stretching activities, and heel inserts and splints. Cortisone injections may be necessary to achieve satisfactory healing and retard inflammation. In later stages of the rehabilitation process, typically after the first week, ice should be discontinued and replaced with heat and massage.

Surgical Treatment
In cases that do not respond to any conservative treatment, surgical release of the plantar fascia may be considered. Plantar fasciotomy may be performed using open, endoscopic or radiofrequency lesioning techniques. Overall, the success rate of surgical release is 70 to 90 percent in patients with plantar fasciitis. Potential risk factors include flattening of the longitudinal arch and heel hypoesthesia as well as the potential complications associated with rupture of the plantar fascia and complications related to anesthesia.